

- Previous Anal Abscess: Most anal fistulas develop following an infection that creates an abscess in the anal glands.
- Crohn’s Disease: This inflammatory bowel condition increases the likelihood of developing fistulas due to chronic inflammation of the intestinal tract.
- Previous Trauma: Injury to the anal area, including surgical procedures or childbirth complications, can lead to fistula formation.
- Radiation Therapy: Patients who receive radiation treatment to the pelvic area face an increased risk of developing fistulas.
- Tuberculosis: In rare cases, tuberculosis can affect the anal area and result in fistulas.
Anal Fistula Treatment in Singapore
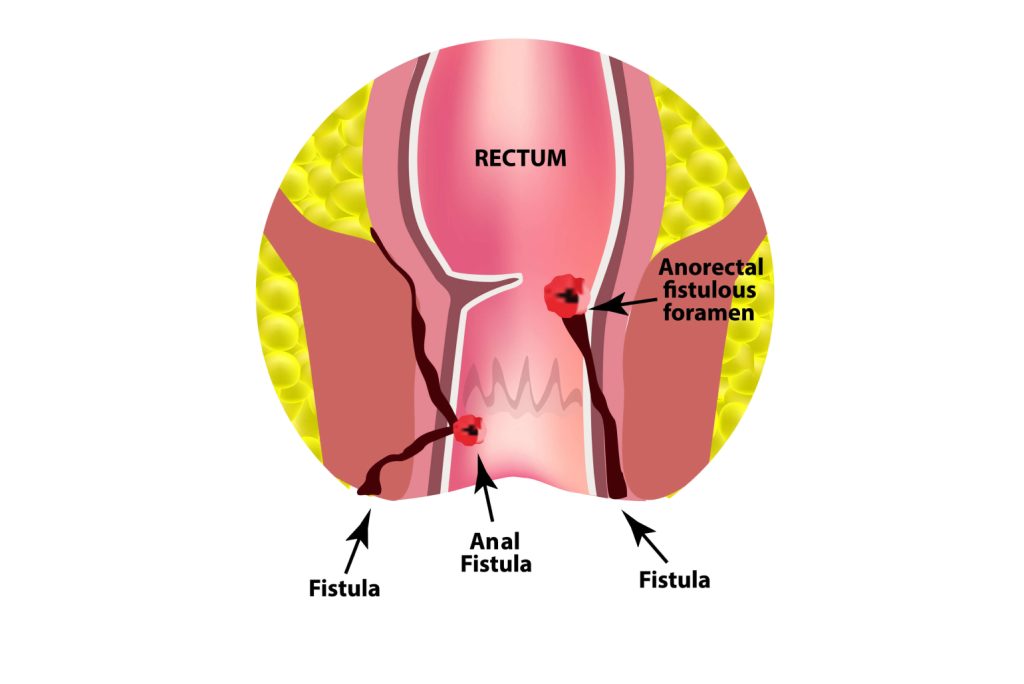
An anal fistula is an abnormal passageway connecting the anal canal (the internal part of the anus) to the skin near the anus. This condition usually arises after an anal abscess (a localised infection) fails to heal completely, resulting in a tunnel that remains infected. This tunnel enables bacteria and waste materials to collect, leading to recurring infections, fluid discharge, and irritation, which can disrupt everyday activities and require medical treatment.

Symptoms of an Anal Fistula
Patients with anal fistulas typically experience several distinct symptoms that may vary in intensity and frequency.
- Pain and Swelling: Persistent discomfort and tenderness around the anal area, which often intensifies during bowel movements or prolonged sitting.
- Discharge: Continuous or intermittent drainage of pus or bloody fluid from an opening near the anus, which may have an unpleasant odour caused by bacterial infection in the tract.
- Skin Irritation: Redness and soreness of the skin around the anal area due to constant moisture and irritation from the discharge.
- Recurrent Abscesses: Formation of painful, swollen pockets of infection that may repeatedly develop if the fistula remains untreated.
- Bleeding: Small amounts of blood may appear on toilet paper or in undergarments due to irritation of the fistula tract.
Causes and Risk Factors
Several underlying conditions and factors can contribute to the development of anal fistulas. These include:
Types of Anal Fistula
Anal fistulas in Singapore are grouped based on their location and how they pass through or around the anal sphincter muscles.
Intersphincteric Fistula
This is the most common type. The fistula runs between the internal and external sphincter muscles, connecting the anal canal to the skin near the anus. It usually responds well to surgery.
Transsphincteric Fistula
The fistula passes through both the internal and external sphincter muscles. Treating these requires careful planning to avoid harming the sphincter muscles, which could affect bowel control. In complex cases, the tract may have additional branches.
Suprasphincteric Fistula
This type starts at the anal canal, goes above the sphincter muscles, and then curves back down to the skin. Its complex path makes it more challenging to treat surgically.
Extrasphincteric Fistula
This is the most complicated type. The fistula begins outside the sphincter muscles, passes through a deeper muscle called the levator ani, and then connects to the skin. These usually result from other conditions, such as Crohn’s disease or complications from surgery or radiation therapy.
Diagnostic Methods
Physical Examination
The doctor performs a thorough external inspection and digital rectal examination. This allows identification of external openings and assessment of internal anatomy. The examination may include gentle probing of the fistula tract to determine its course.
MRI Scan
Magnetic Resonance Imaging provides detailed images of the anal and rectal area. The scan shows the precise path of the fistula tract, any branches, and its relationship to surrounding muscles.
Endoanal Ultrasound
This specialised ultrasound technique uses a small probe inserted into the anal canal. It creates detailed images of the anal sphincter muscles and can identify the internal opening of the fistula. The procedure helps assess sphincter muscle integrity before surgery.
Fistulography
The doctor injects contrast material into the external opening of the fistula. X-ray imaging then reveals the path of the fistula tract. This technique can be used when other imaging methods have failed to produce clear results.
Treatment Options
The treatment approach for anal fistulas depends on the type, location, and complexity of the fistula, as well as any underlying conditions.
Non-Surgical Treatment
- Antibiotics: These medications help control infection and reduce inflammation before surgery. A course of antibiotics may temporarily improve symptoms but rarely leads to complete healing of the fistula.
- Seton Placement: A soft thread is passed through the fistula tract and left in place. This technique helps drain the infection and maintain the tract open. Setons may be used as a temporary measure before definitive surgery or as long-term management in complex cases.
- Fibrin Glue: This involves injecting a special adhesive into the fistula tract. The glue fills the tract and seals it from the inside. While less invasive than surgery, success rates vary and the procedure may need to be repeated.
Surgical Treatment
- Fistulotomy: The surgeon opens the entire length of the fistula tract, removes infected tissue, and allows it to heal from the inside out. This procedure works best for simple fistulas that do not involve much sphincter muscle.
- LIFT Procedure: Ligation of Intersphincteric Fistula Tract involves identifying the tract between the sphincter muscles, tying it off, and removing infected tissue. This technique preserves sphincter function and reduces healing time.
- Advancement Flap: The surgeon creates a flap of tissue from the rectum or around the anus to cover the internal opening of the fistula. This technique proves useful for complex fistulas where sphincter preservation is necessary.
Are Your Symptoms Affecting Your Quality of Life?
Consult our MOH-accredited specialist for an accurate diagnosis & personalised treatment plan today.

Prevention and Management
Proper hygiene, including regular cleaning of the anal area and keeping it dry, can help prevent infection and reduce abscess formation. For individuals with conditions like Crohn’s disease, managing the underlying condition through appropriate treatments and lifestyle changes, such as adopting an anti-inflammatory diet and avoiding smoking, is necessary in reducing the risk of fistula recurrence. Ensuring high-fibre intake and staying hydrated can promote regular bowel movements, minimising strain on the anal region.
Frequently Asked Questions
Can anal fistulas heal without surgery?
While antibiotics and other non-surgical treatments may temporarily improve symptoms, most anal fistulas require surgical intervention for complete healing. Spontaneous healing is rare due to the presence of ongoing infection and the tunnel-like nature of the tract.
How long does recovery take after fistula surgery?
Recovery typically takes 6-8 weeks for simple fistulas treated with fistulotomy. Complex procedures may require 8-12 weeks or longer for complete healing. Most patients can return to work within 2-4 weeks, depending on their occupation and the type of surgery performed.
Will the fistula return after treatment?
Recurrence rates depend on various factors, including the type of fistula, surgical technique used, and presence of underlying conditions. Simple fistulas treated with appropriate surgery have recurrence rates under 10%. Complex fistulas or those associated with Crohn’s disease may have higher recurrence rates.
Partnered Programmes & Insurance Plans
For Singaporeans, Singapore Permanent Residents and Foreigners. Please speak to our friendly clinic staff about using your insurance plans.



















contact us
Please leave us a message and our friendly clinic staff will get back to you as soon as possible. For urgent or same day appointments, kindly call the clinic to arrange an appointment.
Our Clinic Locations

Ark Surgical Practice – Mount Elizabeth Medical Centre
3 Mount Elizabeth, #09-07
Singapore 228510
Monday to Friday: 9am – 5pm
Saturday: 9am – 12:30pm
Sunday & Public Holidays: Closed
Ark Surgical Practice – Mount Alvernia Hospital
820 Thomson Road,
Mount Alvernia Hospital, #06-52,
Medical Centre D, Singapore 574623
Wednesday: 9am – 12:30pm
Thursday: 2pm – 5pm
Related Articles
